Abortion is the termination of human pregnancy, often performed in the first 28 weeks of pregnancy. In 1973, the United States Supreme Court in Roe v. Wade recognized a constitutional right to obtain an abortion without excessive government restriction, and in 1992 the Court in Planned Parenthood v. Casey invalidated restrictions that create an undue burden on people seeking abortions. Since then, there has continued to be an abortion debate in the United States, and some states have passed laws in the form of regulation of abortions but which have the purpose or effect of restricting its provision. The proponents of such laws argue they do not create an undue burden.[1] Some state laws that impact the availability of abortions have been upheld by courts. In 2022, Roe and Casey were overturned by the Supreme Court in Dobbs v. Jackson Women's Health Organization, meaning that states may now regulate abortion in ways that were not previously permitted.
Abortion clinic regulations

An abortion clinic is a medical facility that provides abortions. Abortion clinics may be private or public medical practices or nonprofit organizations. In 27 major cities, and much of rural America, most people live 100 miles or more from an abortion clinic.[2]
Regulations for abortions in the United States include state licensing requirements, federal workplace safety requirements, and association requirements. Abortion clinics may also self-impose more stringent requirements than what these regulations require.
Post Roe v. Wade, many states have passed TRAP (Targeted Regulation of Abortion Providers) laws. These regulations are designed to limit the number of abortions performed by decreasing the number of facilities permitted to perform abortions.
One example of a TRAP law is a requirement which states that doctors performing abortions must have admitting privileges at a nearby hospital.[3] Local hospitals may choose to deny admitting privileges to medical professionals if the medical professional is known to be an abortion provider. Critics of admitting privileges laws and other TRAP laws include the American College of Obstetricians and Gynecologists, the American Public Health Association, and the American Medical Association, which have argued that such laws are medically unnecessary and that abortion is already "very safe" in the United States.[4][5]
In 2011, the crimes of Kermit Gosnell, a physician who ran an abortion clinic in Philadelphia, spurred federal and state bills to more strictly regulate abortion facilities. Opponents of the restrictions questioned whether stricter regulations would have deterred Gosnell, who was alleged to be knowingly in violation of existing regulations.[6]
Following the passage of a 2013 Wisconsin law requiring abortion providers to have admitting privileges at a nearby hospital, three Catholic hospital systems in the state intended to deny admitting privileges to abortion providers. Wisconsin's attorney general said this intent violated the Church Amendment of 1973, which prohibits hospitals from receiving federal funds from discriminating against a doctor on the basis of whether the doctor provides abortions.[7]
In 2015, an Arkansas law required a physician who sought to provide an abortion pill to contract another physician who had admitting privileges at a nearby hospital. As a result, no providers could offer medication abortions in Arkansas and two Planned Parenthoods within the state cancelled their abortion services. Critics argued that no evidence was presented that hospital admitting privileges improve the safety of abortions.[8]
In March 2016, Whole Women's Health v Hellerstedt was heard by the Supreme Court. Over eighty amicus curiae briefs were filed with the Court. The case was decided on June 27, 2016, and was reversed and remanded, 5–3, in an opinion by Justice Breyer.[9] In summary, the Supreme Court ruled that Texas cannot place restrictions on the delivery of abortion services that create an undue burden for women seeking an abortion.
In March 2020, the Supreme Court decided in a 5–4 to reverse a lower court's ruling of allowing a Louisiana law to take effect in which abortion clinics required admitting privileges within 30 miles.[10][6]
In June 2020, the Supreme Court held in June Medical Services LLC v Russo that a Louisiana law requiring physicians who perform abortions to have admitting privileges at a local hospital was unconstitutional, and confirmed the Supreme Court's ruling in Whole Woman's Health v. Hellerstedt.[11]
Federal funding of abortions
The Hyde Amendment bars the use of federal funds to pay for abortion except to save the life of the pregnant woman, or if the pregnancy arises from incest or rape.[12][13] Before the Hyde Amendment took effect in 1980, an estimated 300,000 abortions were performed annually using federal funds.[14] The provision withholds federal Medicaid funding of abortions, which impacts especially low-income families.[15] The cost of an abortion weighs heavily on many women. Medicaid funding laws hinder a woman's ability to obtain an abortion. Medicaid funding laws prevent the use of state funds to pay for abortions for disadvantaged women. Medicaid funding restrictions decrease a state's abortion ratio by 39.76% per every one thousand pregnancies.[16]
Laws targeting methods of practice
On 18 April 2007, the U.S. Supreme Court upheld the Partial-Birth Abortion Ban Act that banned abortions in the second trimester, which medical doctors say is the safest time for an abortion to protect the women's health. The Court's decision overturned more than 30 years of precedent.[15] However, throughout the United States, various states have implemented Targeted Regulations of Abortion Providers (TRAP) laws and other classifications of restrictions on bodily autonomy. These laws aim to reduce the rate of abortions and limit access to medical providers, which has been proven to be less effective than anticipated in various research reviews. Researchers find the methods of TRAP laws to be practical concerning the variables of loss in opportunity and potential costs but the impacts on abortion demand are otherwise insufficient.[17] Some states have also successfully limited abortion access to specific periods and circumstances: laws banning abortion before 13 weeks, between 13 and 24 weeks, bans on particular reasons for abortion (genetic disorders or health issues).[18]
Abortion restrictions generate the threat of legal risks among clinicians and other medical professionals and impact the quality of care and treatments for the individuals residing in restrictive states. Based on a survey conducted by the Kaiser Family Foundation (KFF) that concentrates on responses of OBGYNs and their reproductive health services, the research found that their decision-making autonomy, the ability to practice within the standard of care, and provider-patient relationships have been depreciated by the Dobbs decision and the oppressive state restrictions.[19] Additional descriptions of existing restrictive laws on methods of practice include gestational limits, state-required waiting periods, parental involvement for minors who are undergoing pregnancy, the prohibition of the use of state funds for abortions, and the lack of insurance coverage in medical insurance plans.[20]
Mandatory ultrasounds
Ultrasounds are not medically necessary for abortions; however, some states require physicians to perform an ultrasound, and some require the people seeking an abortion to view the ultrasound and listen to the fetus's heartbeat if any. As of May 2019, twelve states required people seeking an abortion to have an ultrasound before being allowed to have the procedure. This number was 26 in September 2020. 14 states required people to be issued with ultrasound information in May 2019.[21] Mandatory transvaginal ultrasounds have been particularly controversial.[22] In Texas, for instance, even if previous ultrasounds had indicated severe congenital defects, a person seeking an abortion was required under a 2012 law to have another ultrasound done, "administered by [their] abortion doctor, and [they had to] listen to a state-mandated description of the fetus [they were] about to abort", though state-issued guidelines later eliminated the ultrasound requirement if the fetus had an "irreversible medical condition".[23] Some states require people to seek counseling after the ultrasound to determine if they would like to continue with an abortion.
On November 12, 2013, the U.S. Supreme Court declined to hear an appeal by the state of Oklahoma to the overturning of a bill that mandated compulsory ultrasound examinations.[24]
Waiting periods
27 states require a person seeking an abortion to wait up to six days, most often 1 day, although one state requires a waiting period of eighteen hours while another requires a waiting period of seventy-two hours [25] after receiving counseling and before having the abortion.[26] 14 states require the person to make two trips to the clinic before receiving an abortion as they must receive counseling in person at the clinic, wait the designated waiting period, and return to the clinic to have the procedure done.[27] South Dakota requires the person to obtain mandatory counseling from an anti-abortion crisis pregnancy center during this time frame.[28] Waiting periods are put in place to allow women to consider all their options. as of 2013 10 states had two-visit laws. These laws require women to receive mandatory counseling in person at least twenty-four hours before their abortion procedure making women go to two appointments to obtain an abortion.[29]
Six-week bans
A six-week abortion ban, also called a "fetal heartbeat bill" by proponents, is a law in the United States which makes abortion illegal as early as six weeks gestational age (two weeks after a woman's first missed period), which is when proponents falsely claim that a "fetal heartbeat" can be detected.[30][31][32] Medical and reproductive health experts, including the American Medical Association and the American College of Obstetricians and Gynecologists, say that the reference to a fetal heartbeat is medically inaccurate and intentionally misleading[33][34][35][36][37][38] because a conceptus is not called a fetus until eight weeks after fertilization, as well as that at four weeks after fertilization, the embryo has no heart, only a group of cells which will become a heart.[39][40][41][42][43] Medical professionals advise that a true fetal heartbeat cannot be detected until around 17 to 20 weeks of gestation when the chambers of the heart have become sufficiently developed.[43]
Janet Porter, an anti-abortion activist from Ohio, is considered to be the person that first authored this type of legislation.[44] Efforts to introduce her model law succeeded in passing through political branches of government in about a dozen states, but in most cases the courts struck down or blocked similar legislation. However, the Texas law and analogues subsequently adopted in other states succeeded due to a unique enforcement mechanism that makes challenging the law extremely difficult, and which was upheld by the Supreme Court. In some states, the heartbeat bills' effect (whether blocked or not) has been minimized by more stringent total abortion bans that were announced following the decision in Dobbs v. Jackson Women's Health Organization; in other states, such as Ohio,[45] South Carolina and Tennessee, judges lifted the injunctions against the previously passed laws.
Porter's anti-abortion group argues that a heartbeat "is the universally recognized indicator of life".[46] Reproductive rights advocates, on the other hand, say that these bans are de facto complete abortion bans, since many women do not even know that they are pregnant six weeks after their last menstruation, which is four weeks post-fertilization.[30][39][47]Status of most restrictive states
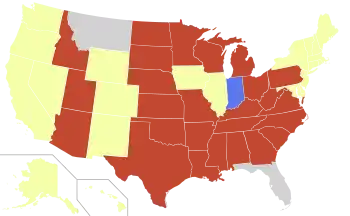
The Guttmacher Institute has designated 12 states as being having the most restrictive abortion restrictions.[48]
- Alabama
- Arkansas
- Idaho
- Kentucky
- Louisiana
- Mississippi
- Missouri
- Oklahoma
- South Dakota
- Tennessee
- Texas
- West Virginia
Physician scripts
Some states require a doctor to read a prepared script to the person seeking an abortion to secure informed consent. These scripts may include medically inaccurate information intended to persuade the patient not to have an abortion, such as the claim that the abortion will increase the risk of breast cancer or of psychological problems, which are not supported by mainstream medical organizations or scientific consensus.[23][49] As of July 2013, 12 states require that women be given information on the ability of a fetus to feel pain.[50] In Planned Parenthood v. Rounds, the Eighth Circuit Court of Appeals ruled that a South Dakota law requiring doctors to give patients false or misleading information about the suicide risk in women who have abortions was not unconstitutional.[51] Alaska, Kansas, Mississippi, Oklahoma, and Texas mandate that before an abortion can be performed, the patient must be counseled on the link between abortion and breast cancer.[26] There is currently no evidence from scientific research that abortion has the ability to cause breast cancer.[52] Kansas, Louisiana, Mississippi, Nevada, North Carolina, South Dakota, Texas, and West Virginia mandate that patients receive counseling on the potential psychological impacts of abortion on the person who receive them before an abortion can be given.[26] Five states require that an abortion patient is counseled that personhood begins at conception.[27]
Liability
Physicians can be liable for the abortion of a fetus if the right procedures are not taken. Doctors should inform every patient of all material risks of the procedure. The doctors can not give a small number of details to the patient but everything that will be done must be presented.[53] A 1997 Louisiana law creates a civil cause of action for abortion-related damages, including damage to the unborn, for up to ten years after the abortion. The same law also bars the state's Patient's Compensation Fund, which limits malpractice liability for participating physicians, from insuring against abortion-related claims.[54][55] An attorney for the Center for Reproductive Rights, which opposes the law, said the law is an attempt to drive abortion providers out of practice, and that every completed abortion imposes strict liability under the law because abortion necessarily involves damage to the unborn.[56]
Reporting
As of 2010, 46 of 50 states and the District of Columbia had either mandatory or voluntary reporting of abortion statistics. According to an associate of the Guttmacher Institute, reporting requirements were generally "benign" and treated confidentially, but the requirements in some states have become more intrusive.[57]
A 2009 Oklahoma law, overturned by a federal court in 2010, would have required doctors to report information from a 37-question form about every person receiving an abortion to the state health department for publication in an online registry.[57] A lawyer for the Center for Reproductive Rights, a co-plaintiff in the lawsuit challenging the law, said the law would have made public potentially identifying details about the people, and was intended to dissuade people from seeking abortions.[58] Todd Lamb, the state senator who sponsored the law, called it "essential in protecting the sanctity of life" and "pro-life".[57]
Transportation Issues to accessing abortion
In states such as Alabama and Mississippi people often have the challenge of traveling far distances to obtain a medical abortion. As of 2019, there are only three healthcare clinics in Alabama that offer abortion. According to Guttmacher Institute, about one-third of people seeking an abortion in Alabama must travel more than 25 miles to receive the procedure.[59] Furthermore, only seven percent of counties in Alabama have a medical provider in the county that offers abortion.[59]
People often must seek two trips to an abortion provider due to a waiting period. The waiting period is typically 48 hours before the scheduled abortion. Organizations such as Yellowhammer Fund, help people seeking an abortion. They provide financial costs and transportation for women in Alabama, Mississippi, and the Florida panhandle area. On the other hand, most clinics do not offer transportation or financial resources to patients. Most of the time, it is the responsibility of a patient to find their means of transportation and finances to fund the abortion.[59]
Access to abortion and other reproductive health procedures in the United States varies among specific state policies, and they are usually provided in separate facilities other than hospitals. However, due to changes in restrictions in certain states, many individuals have to travel across state lines to obtain the care they require. For example, according to research from the CDC, an average of 8% of patients have left their state of residence for abortion care, and overall, 71% of patients have traveled from a state with restrictive policies.[60] While it might seem somewhat affordable to travel across the states for reproductive healthcare, it has created a significant burden on those who have low incomes or have dealt with other forms of systemic oppression. The rise of stigma and prejudices against those who need abortion care have caused an incline in emotional and mental strain, which can also impact an individual's well-being and decisions. The geographical locations of abortion facilities and accessibility impact the general demand of abortion by reducing search costs, travel time, and travel expenses.[61]
Language barriers and immigrant issues related to abortion
An issue that can arise among non-native English speakers or immigrant people is the lack of access to a translator while attempting to seek an abortion. Under federal law, citing the Title VI of the Civil Rights Act of 1964 and the Affordable Care Act requires that providers who receive federal funding provide an oral interpreter and translated material.[62] According to the American Civil Liberties Union, in 1976, Congress passed a bill called the Hyde Amendment which purposely excludes abortion from being included in healthcare services provided to people through Medicaid.[62] The only exception to this rule is if a person's life is in danger due to pregnancy, cases of rape or incest, illness, or injury. This results in many healthcare clinics that offer abortion, not being able to accommodate non-English speaking patients. Due to the limitations set by the federal government. There are limited resources for non-English speaking patients when it comes to abortion.[62]
Additionally, when it comes to organizations such as the United States Immigration and Customs Enforcement (ICE), abortion is heavily regulated. ICE complies with the Hyde Amendment from 1976, and only offers abortion for reasons related to incest, rape, or the endangerment of a mother's life due to pregnancy.[63] According to the National Latina Institute for Reproductive Justice, around 80% of women attempting to enter the United States through illegal means, get sexually assaulted. Thus, a high number of women in ICE detention centers often seek medical abortions. Furthermore, there have been proposals by Alabama Representative Robert Aderholt to attempt to allow ICE employees to refuse to conduct an abortion.[63] Such proposals have so far not passed in congress. Under the Trump administration, minors who were held in ICE custody were unable to seek an abortion. According to PBS, a federal appeals court ruled against the Trump administration on June 14, 2019. The three federal judges cited that the Trump administration could not regulate a minor's decision to receive a medical abortion.[63] Furthermore, the policy dates to 2017, when the ban was supposed to take effect. The ban specifically targets immigrant minors attempting to enter the country, which is then held by the United States government for attempting to illegally enter the US. At the time, the Trump administration could have attempted to ask the United States Court of Appeals to hear the case, but that seems to have never gone through.[63]
Impact of the COVID-19 pandemic on access to abortion
In March 2020, COVID-19 impacted the United States, and the CDC declared COVID-19 a pandemic. During this time, numerous states began issuing orders to postpone any non-essential medical products, specifically abortion.[64][65] Texas restricted abortion access on March 23, 2020, citing that a temporary ban on non-essential medical services was necessary to curb the COVID-19 pandemic.[65] In the following weeks, more states such as Ohio, Alabama, Iowa, and Oklahoma followed Texas in the same ban on non-essential produces. In a press conference on March 27, 2020, Iowa Governor Kim Reynolds clarified that surgical abortion procedures would be included in the temporary hold on all non-essential surgeries.[66]
The Supreme Court accepted a request from the Food and Drug Administration to ban medical providers from sending mifepristone (the “abortion pill”) via mail.[67] This pill is primarily used for ending pregnancies that are within the first trimester. The rule was suspended by a federal judge in the summer of 2020 due to the ongoing pandemic.[67] The reinstated rule forces people seeking an abortion to go into a medical provider's office and have an in-person visit to receive the pill. The Food and Drug Administration attempted to appeal the original decision on August 26, 2020, to the Supreme Court. The Supreme Court responded with a denial to the Food and Drug Administration to overturn the order. The Supreme Court cited that the Food and Drug Administration needed to provide more information as to why Judge Chuang's order needed to be overturned. Finally, on January 12, 2021, the Trump Administration submitted a more detailed request, which was granted by the Supreme court to lift the suspension on not requiring in-person visits and mailing of the abortion pill.[67]
Limitations for minors under 18
In around 37 states, a parental figure is required to have a say in a minor's decision related to abortion. More specifically, parental consent laws require an unmarried minor to obtain consent from a parent or judge.,[68] in 27 states, one or both parents are required to give their permission to the minor. By age twenty, 40 percent of teenage women have been pregnant, 84% of which are unintended.[69] Ten states require both parents to consent to medical abortion. Furthermore, a minor may not have the finances or transportation to seek an abortion. Since most minors are labeled as dependent on their parents' or guardians' tax forms, they most likely do not have the money to obtain an abortion. Also, if the minor is on their guardian's insurance, the guardian has access to the health insurance and information of the minor. It is estimated that around 350,000 United States teenagers under the age of 18 become pregnant each year. Of that population, around 31% of them have a medical abortion.[70]
Insurance limitations
In twelve states, private insurance is restricted from covering abortion under their plans. In most cases, insurance only covers abortion if a person's life is endangered by a medical professional. If an underinsured or uninsured person seeks an abortion, they may need to pay out-of-pocket costs to receive the treatment needed. These limitations of the lack of insurance coverage greatly affect mostly low-income minorities. The average "abortion pill" cost around US$500. On top of that, under the Affordable Care Act passed in 2010 by congress, abortion is not required to be covered under the ten essential coverages. Government-run health insurance, such as Medicaid, can provide coverage for medical abortion.[71]
See also
References
- ↑ "undue burden". LII / Legal Information Institute. Retrieved 2021-04-07.
- ↑ "10 things you need to know about abortion laws in the US". www.amnesty.org. 11 June 2019. Retrieved 2021-04-07.
- ↑ "Abortion, Hospital Admitting Privileges, and Whole Woman's Health v. Cole" (PDF). Retrieved October 1, 2015.
- ↑ Grossman, Daniel; Baum, Sarah; Fuentes, Liza; White, Kari; Hopkins, Kristine; Stevenson, Amanda; Potter, Joseph E. (November 2014). "Change in abortion services after implementation of a restrictive law in Texas". Contraception. 90 (5): 496–501. doi:10.1016/j.contraception.2014.07.006. PMC 4179978. PMID 25128413.
- ↑ "Opposition to Requirements for Hospital Admitting Privileges and Transfer Agreements for Abortion Providers". APHA Policy Statement. Retrieved 14 March 2016.
- 1 2 Caplan-Bricker, Nora (May 1, 2013). "The Kermit Gosnell Effect". The New Republic.
- ↑ Ahmed, Akbar (August 7, 2013). "Hospitals can't deny admitting privileges to abortion doctors, AG says". Milwaukee Journal Sentinel. Retrieved October 4, 2013.
- ↑ "Medication Abortion". The Henry J. Kaiser Family Foundation. 2018-06-01. Retrieved 2020-05-09.
- ↑ "Whole Woman's Health v. Hellerstedt". SCOTUSblog. Retrieved 2020-04-27.
- ↑ Sheppard, Kate (June 27, 2011). "Abortion Foes' Latest Backdoor Ban". Mother Jones.
- ↑ "Russo v. June Medical Services LLC". SCOTUSblog. Retrieved 2020-04-27.
- ↑ "Abortion Funding Ban Has Evolved Over The Years". NPR.org. Retrieved 2019-03-10.
- ↑ "The Hyde Amendment at 35: A new abortion divide - the Washington Post". The Washington Post. Archived from the original on March 7, 2016. Retrieved February 23, 2016.
- ↑ Rovner, Julie (15 December 2009). "Abortion Funding Ban Has Evolved Over The Years". National Public Radio Inc. Retrieved 7 June 2019.
- 1 2 "Federal and State Bans and Restrictions on Abortion". www.plannedparenthoodaction.org. Retrieved 2021-04-08.
- ↑ Medoff, Marshall H. 2010. "State Abortion Policies, Targeted Regulation of Abortion Provider Laws, and Abortion Demand." Review of Policy Research 27 (5): 577-594.
- ↑ Medoff, Marshall H.; Dennis, Christopher (2011-01-01). "Public Preferences, Political Party Control, and Restrictive State Abortion Laws". American Review of Politics. 31: 307–331. doi:10.15763/issn.2374-7781.2010.31.0.307-331. ISSN 2374-779X.
- ↑ Szastok, Marta; Kossowska, Małgorzata; Pyrkosz-Pacyna, Joanna (2019-05-15). "Women Can't Have It All: Benevolent Sexism Predicts Attitudes Toward Working (vs. Stay-at-Home) Mothers". Social Psychological Bulletin. 14 (1). doi:10.32872/spb.v14i1.29461. ISSN 2569-653X.
- ↑ Weigel, Gabriela; Frederiksen, Brittni; Ranji, Usha; Salganicoff, Alina (2022-06-01). "Screening and Intervention for Psychosocial Needs by U.S. Obstetrician-Gynecologists". Journal of Women's Health. 31 (6): 887–894. doi:10.1089/jwh.2021.0236. ISSN 1540-9996. PMID 34995169. S2CID 245815444.
- ↑ Beckman, Linda J (February 2017). "Abortion in the United States: The continuing controversy". Feminism & Psychology. 27 (1): 101–113. doi:10.1177/0959353516685345. ISSN 0959-3535. S2CID 151395674.
- ↑ "State Ultrasound Requirements in Abortion Procedure". The Henry J. Kaiser Family Foundation. 28 May 2019. Retrieved 15 March 2020.
- ↑ Sheppard, Kate (March 5, 2012). "Mandatory Transvaginal Ultrasounds: Coming Soon to a State Near You". Mother Jones.
- 1 2 "'We Have No Choice': A Story Of The Texas Sonogram Law". NPR. January 22, 2013.
- ↑ Court lets stand an Oklahoma ruling that a state abortion law is unconstitutional', Washington Post, Juliet Eilperin, 12 November 2013. Retrieved 12 November 2013.
- ↑ Medoff, Marshall H. 2013. "Social Policy and Abortion: A Review of the Research." Open Demography Journal 6: 18-27. http://dx.doi.org/10.2174/1874918601306010018/
- 1 2 3 "An Overview of Abortion Laws". Guttmacher Institute. 2016-03-09. Retrieved 2020-05-09.
- 1 2 "Counseling and Waiting Periods for Abortion". Guttmacher Institute. 2016-03-14. Retrieved 2020-05-09.
- ↑ "South Dakota governor signs extended abortion wait period law". Reuters. 2013-03-08. Retrieved 2020-05-09.
- ↑ Medoff, Marshall H. 2013. "Social Policy and Abortion: A Review of the Research." Open Demography Journal 6: 18-27. http://dx.doi.org/10.2174/1874918601306010018
- 1 2 Glenza, Jessica (June 7, 2019). "Why the Guardian is changing the language it uses to describe abortion bans". The Guardian. ISSN 0261-3077. Retrieved June 7, 2019.
ACOG, which represents 58,000 physicians, says the term 'heartbeat bill' is not medically accurate. 'Pregnancy and fetal development are a continuum,' said the ACOG president, Dr Ted Anderson. 'What's interpreted as a heartbeat in these bills is actually electrically induced flickering of a portion of fetal tissue that will become the heart as the embryo develops.' ... The bans, dubbed "heartbeat" bills by supporters, have the practical effect of banning abortion before most women know they are pregnant.
- ↑ Gordon, Mara (5 June 2019). "Early Abortion Bans: Which States Have Passed Them?". NPR. Retrieved 12 May 2022.
- ↑ Glenza, Jessica (June 5, 2019). "Doctors' organization: calling abortion bans 'fetal heartbeat bills' is misleading". The Guardian. ISSN 0261-3077. Retrieved June 7, 2019.
- ↑ McDonald, Jessica (July 26, 2019). "When Are Heartbeats Audible During Pregnancy?". FactCheck. Retrieved May 7, 2022.
- ↑ Carr Smyth, Julie; Kruesi, Kimberlee (May 14, 2021). "'Fetal heartbeat' in abortion laws taps emotion, not science". AP News. Associated Press. Retrieved May 7, 2022.
- ↑ Feibelò, Carrie; Simmons-Duffin, Selena (February 9, 2021). "The Texas Abortion Ban Hinges On 'Fetal Heartbeat.' Doctors Call That Misleading". NPR. Retrieved May 7, 2022. Updated May 3, 2022.
{{cite web}}: CS1 maint: postscript (link) - ↑ Irvine, Bethany (September 2, 2021). "Why 'heartbeat bill' is a misleading name for Texas' near-total abortion ban". The Texas Tribune. Retrieved May 6, 2022.
- ↑ Heaney, Kate (May 24, 2019). "Why 'Fetal Heartbeat Bill' is a Misleading Phrase – Embryos Don't Have Hearts". The Cut. Retrieved May 6, 2022.
But obstetricians say the term 'fetal heartbeat' is misleading, and that this scientific misunderstanding, among countless others, may contribute to negative public opinion toward abortion. To wit: though pulsing cells can be detected in embryos as early as six weeks, this rhythm — detected by a doctor, via ultrasound — cannot be called a 'heartbeat,' because embryos don't have hearts. What is detectable at or around six weeks can more accurately be called 'cardiac activity,' says Robyn Schickler, OB/GYN and fellow with Physicians for Reproductive Health. The difference between 'cardiac activity' and 'heartbeat' may seem linguistically minimal, but Schickler and others argue otherwise. At this stage, she says, what doctors can detect is essentially communication between a group of what will eventually become cardiac cells.
- ↑ Baran, Nicole M.; Goldman, Gretchen; Zelikova, Jane (August 21, 2019). "Abortion Bans Based on So-Called 'Science' Are Fraudulent". Scientific American. Retrieved May 7, 2022.
So-called heartbeat bills, which ban abortion as early as after six weeks of pregnancy, are not based on science. In fact, no heart yet exists in an embryo at six weeks. Yet six states and counting enacted such bills in 2019, in addition to Alabama's near-total ban. ... Both heartbeat bills and abortion reversal laws have been opposed by leading medical groups, including the American Medical Association and the American College of Obstetricians and Gynecologists.
- 1 2 Rogers, Adam (May 14, 2019). "'Heartbeat' Bills Get the Science of Fetal Heartbeats All Wrong". Wired. Retrieved May 23, 2019.
Using the word heartbeat here is an intentional obfuscation," [Jennifer Kerns, an ob-gyn at UC San Francisco and director of research in obstetrics and gynecology at Zuckerberg San Francisco General Hospital] says. "Hearing the word heartbeat plays upon people's emotions … when in fact what it does is effectively ban abortions for many people, because many people don't even know they're pregnant at six weeks.
- ↑ Belluck, Pam (May 9, 2019). "What Do New State Abortion Laws Really Mean for Women?". The New York Times. ISSN 0362-4331. Retrieved May 18, 2019.
According to the American College of Obstetricians and Gynecologists, an embryo is not considered a fetus until eight weeks after fertilization, which is about 10 weeks into a pregnancy. At six weeks into a pregnancy, the tissues that will become the heart are beginning to develop and a pulsing can be detected that is faster than the heartbeat of the expectant mother. Several medical experts, including those opposed to the new abortion restrictions, say that it isn't medically correct to call that pulsing a heartbeat. Rather, they say, it is the vibration or "embryonic cardiac activity" of the fetal pole, a tubelike structure that will become the heart.
- ↑ Baker, Carrie N. (September 7, 2021). "Media Repeat Junk Science Behind Abortion Ban Laws: Check the Science—There is No Heartbeat at Six Weeks". Ms. Retrieved May 7, 2022.
The Texas law bans abortion at six weeks of pregnancy, which is around four weeks after fertilization — when an embryo is the size of grain of rice. At this point in pregnancy, the embryo develops a group of cells that gain the capacity to fire electrical signals, described by Dr. Saima Aftab as "a little flutter in the area that will become the future heart." ... This electrical signal can only be detected by a highly sensitive ultrasound device.
- ↑ Simmons-Duffin, Selena; Feibel, Carrie (2022-05-02). "The Texas Abortion Ban Hinges On 'Fetal Heartbeat.' Doctors Call That Misleading". NPR.
The term "fetal heartbeat," as used in the anti-abortion law in Texas, is misleading and not based on science, say physicians who specialize in reproductive health.
- 1 2 "ACOG Guide to Language and Abortion". American College of Obstetricians and Gynecologists. Retrieved 2022-05-16.
"Heartbeat bill" - It is clinically inaccurate to use the word "heartbeat" to describe the sound that can be heard on ultrasound in very early pregnancy. In fact, there are no chambers of the heart developed at the early stage in pregnancy that this word is used to describe, so there is no recognizable "heartbeat." What pregnant people may hear is the ultrasound machine translating electronic impulses that signify fetal cardiac activity into the sound that we recognize as a heartbeat. "Fetal heartbeat" - Until the chambers of the heart have been developed and can be detected via ultrasound (roughly 17-20 weeks of gestation), it is not accurate to characterize the embryo's or fetus's cardiac development as a heartbeat.
- ↑ "For anti-abortion activists, success of 'heartbeat' bills was 10 years in the making". Center for Public Integrity. 2019-06-20. Retrieved 2022-06-26.
- ↑ Knight, Anna Staver and Cameron. "Ohio's six-week abortion ban becomes law hours after Supreme Court's Dobbs decision". The Cincinnati Enquirer. Retrieved 2022-06-26.
- ↑ North, Anna (2019-04-19). "The "heartbeat" bills that could ban almost all abortions, explained". Vox. Retrieved 2022-06-26.
- ↑ Anna North (May 16, 2019). "Abortion is still legal in America". Vox. Retrieved May 23, 2019.
Because that's before many people know they are pregnant, reproductive rights advocates say the "heartbeat" bills are de facto abortion bans
- ↑ "Interactive Map: US Abortion Policies and Access After Roe". states.guttmacher.org. Retrieved 2023-03-02.
- ↑ Lazzarini, Zita (November 20, 2008). "South Dakota's Abortion Script—Threatening the Physician-Patient Relationship". New England Journal of Medicine. 359 (21): 2189–91. doi:10.1056/NEJMp0806742. PMID 19020321.
- ↑ "State Policies in Brief: An Overview of Abortion Laws" (PDF). Guttmacher Institute. Retrieved 2 July 2013.
- ↑ Can the Government Require Doctors to Provide Misleading Information to Patients Seeking Abortions?
- ↑ "Abortion and Cancer Risk". www.cancer.org. Retrieved 2020-05-09.
- ↑ "Abortion, information & the law: what every doctor needs to know". Issues in Law & Medicine. 16 (3): 283–284. 2001. ISSN 8756-8160. PMID 11285863.
- ↑ Cassens Weiss, Debra (September 6, 2013). "5th Circuit finds no undue burden in law curbing liability protection for abortion providers". ABA Journal. Retrieved October 8, 2013.
- ↑ Catalanello, Rebecca (September 5, 2013). "Abortion providers challenging Louisiana law suffer setback at 5th Circuit". Times-Picayune. Retrieved October 8, 2013.
- ↑ Mcconnaughey, Janet (March 29, 2012). "Judge forbids La to enforce abortion liability law". Deseret News. Associated Press. Retrieved October 8, 2013.
- 1 2 3 Donaldson James, Susan (February 19, 2010). "Okla. Strikes Down Law That Would Have 'Undressed' Women". ABC News. Retrieved October 8, 2013.
- ↑ "Oklahoma abortion law to force women to list personal details online". Daily Telegraph. October 19, 2009. Retrieved October 8, 2013.
- 1 2 3 "State Facts About Abortion: Alabama". Guttmacher Institute. 2016-01-26. Retrieved 2021-08-04.
- ↑ Smith, Mikaela H.; Muzyczka, Zoe; Chakraborty, Payal; Johns-Wolfe, Elaina; Higgins, Jenny; Bessett, Danielle; Norris, Alison H. (June 2022). "Abortion travel within the United States: An observational study of cross-state movement to obtain abortion care in 2017". The Lancet Regional Health - Americas. 10: 100214. doi:10.1016/j.lana.2022.100214. ISSN 2667-193X. PMC 9903901.
- ↑ Medoff, Marshall H. (2013-09-25). "Social Policy and Abortion: A Review of the Research". The Open Demography Journal. 6 (1): 18–27. doi:10.2174/1874918601306010018. ISSN 1874-9186.
- 1 2 3 "Public Funding for Abortion". American Civil Liberties Union. Retrieved 2021-08-04.
- 1 2 3 4 "Detained Immigrant Women Are Facing A Grueling Abortion Struggle". National Latina Institute for Reproductive Justice (in Spanish). 2017-05-24. Retrieved 2021-08-04.
- ↑ "Timeline: Our Fight Against Opportunistic Abortion Bans During the COVID-19 Pandemic". www.plannedparenthoodaction.org. Retrieved 2021-08-06.
- 1 2 "Court rules against Trump's abortion policy for immigrant teens in government shelters". PBS NewsHour. 2019-06-14. Retrieved 2021-08-04.
- ↑ Cummings, Caroline (2020-03-27). "Gov. Reynolds office: Order halting non-essential surgeries includes surgical abortions". KGAN. Retrieved 2021-08-04.
- 1 2 3 "Justices grant FDA request to block mail delivery of abortion pills". SCOTUSblog. 2021-01-12. Retrieved 2021-08-04.
- ↑ Haas-Wilson, D. (1993). The economic impact of state restrictions on abortion: Parental consent and notification laws and Medicaid funding restrictions. Journal of Policy Analysis and Management, 12(3), 498. https://doi.org/10.2307/3325303
- ↑ Haas-Wilson, D. (1993). The economic impact of state restrictions on abortion: Parental consent and notification laws and Medicaid funding restrictions. Journal of Policy Analysis and Management, 12(3), 498.https://doi.org/10.2307/3325303
- ↑ "Laws Restricting Teenagers' Access to Abortion". American Civil Liberties Union. Retrieved 2021-08-04.
- ↑ "Coverage for Abortion Services in Medicaid, Marketplace Plans and Private Plans". KFF. 2019-06-24. Retrieved 2021-08-04.
External links
- Distance to the nearest abortion provider for women aged 15–44, 2000–2014, by state or county